
 Svenska
Svenska”Je pense, donc je suis”
Descartes
1) Dopamine and -acetylcholine hypothesis
Dopamine is, according to me, the molecule of life. Giving life a meaning. A sense.
A value. It helps to send you signals if something is good or bad. Pleasure or punishment. Helps you to feel good. Helps you to survive.
But, with some life experience, I have noticed that balance is crucial. There should be something balancing dopamine, and here, acetylcholine can play an important role. This is very complicated since there are so many neurotransmitters and they are all important.
Smoking (and/or other forms of nicotine intake) is very common in several diseases. Professor Arvid Carlsson (Göteborgs Universitet, Sweden) hypothesised in the 1950’s that dopamine is involved in the pathophysiology of eg addiction (Engel and Söderpalm 1999; Yoshida et al 1980), schizophrenia, Parkinson’s disease and Alzheimers disease (?).
Smoking is highly observed among eg alcohol dependent individuals, depression and schizophrenia. These diseases are a huge burden for today’s societies in terms of money, suffering, and not least, for families. During my years at the departement of pharmacology, I always thought about why smoking is so common in several diseases. I never got a good answer.
Several experiments in vivo have demonstrated that dopamine plays a crucial role in these diseases. Professor Arvid Carlsson has further gained evidence for his hypothesis by introducing dopamine stabilisers. A pharmacological substance, with dual effects, acting as an agonist and antagonist depending on the state of the environment; concentration dependent.
However, as seen in Parkinson´s disease, today´s available pharmacological treatment is not optimal. ”On-off” symptoms may be observed.
Dopamine neurons are widely distributed throughout the brain in rather distinct pathways. These neurons are closely located to eg cholinergic neurons. Cholinergic neurons have muscarinic (G-protein coupled) and nicotinic receptors (ion channels). To the best of my knowledge, dopamine neurons do not have ionic receptors. Maybe they are equipped with rapidly responding receptors, but they have not been found or simply, they do not exist.
A possible way to smooth side-effects may be to give more input to dopaminergic activity by cholinergic sparkling eg from the mesopontine area. These cholinergic neurons project to eg the ventral tegmental area and the substantia nigra. It should be noted that this is very difficult to study. Experiments will find out if dopamine and acetylcholine are like ”Yin and Yang”. Opposites, stabilizing each other. Like an old fashion weight, and it is established that overweight is not good for health.
B. Functional nicotinic autoreceptors
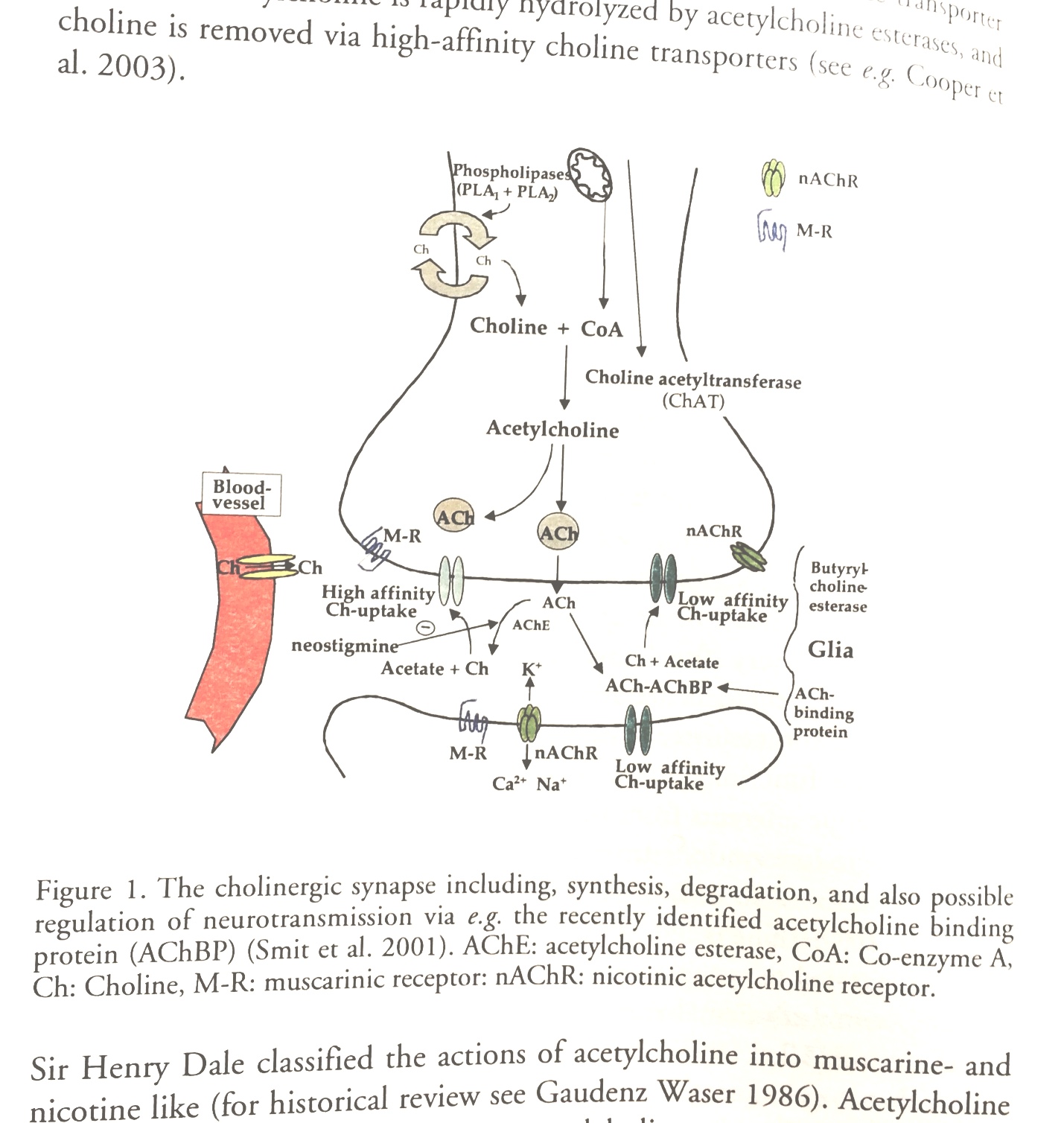
Below is an illustration of a cholinergic synapse. I have previously written about functional nicotinic acetylcholine auto receptors. These receptors should be introduced in this illustration pre-synaptically. Furthermore, I would suggest that these nicotinic receptors are composed by α4* and β2* nicotinic subunits. Here, It would be interesting to listen to Professor Arvid Carlssons comments. I have followed his internet lectures where he discuss dopaminergic auto receptors.
It is interesting to note (now I write from my memory) that in Alzheimers disease, these subunits seem to be associated with the disease.
Remember, this is theoretical pharmacology.
A possible new pharmaceutical treatment, maybe not only in Alzheimers disease, could be to modulate this receptor. Acetylcholine esterase inhibitors are of clinically significantly importance. Increasing acetylcholine activity/concentrations could be of clinical significance.
However, it should be noted that there is some kind of difference between cholinergic and dopaminergic activity. I write this from my gut feeling. Cholinergic activity is more intense, whereas dopaminergic activity is in a way smoother. But they interact in balance. The nicotinic receptor is rapidly desensitized. It needs recovery to refunction. That is probably why many smokers like the first cigarett in the morning. The nicotinic receptors have been in rest over night.
C. Does dendritic dopamine overflow in eg substantial nigra/ventral tegmental area interact with cholinergic neurons to give feed-back? A way to obtain balance between dopaminergic and cholinergic neurons.
Of course I meet many PhD students during studies. And I also learnt a lot about other research areas. I think that, being away from pre-clinical research has matured my thoughts. This has resulted in Dopamine-acetylcholine hypothesis.
There has to be communication between dopamine neurons and acetylcholine neurons. Information must be processed and communicated. “Left hand needs to know what right hand is doing in order to work in harmony”. This will be very difficult to study. In vitro will be the easiest first approach.
2) Prevention of diseases in humans later in life is to monitor ophthalmological status in newborns – to obtain stability in the body.
Since I have read a lot about the brain in the literature a decade ago I have had time to reflect. I believe (a hypothesis that might be rejected) that the development of the ophthalmological nervous system is very important for the brain, our function (personality, decision making, motivation) to be. Both ”eyes” need to be in balance during development. If I remember correctly, the eye nerves cross in approximately in the middle of the brain and projects like a ”spray” in the posterior. ”Our function to be (personality)” is very difficult to define. This also poses a lot of questions. Should personality be defined? Maybe, what is human disappears then.
This should be difficult to explain. Here, I feel, one should be very humble, and it needs careful and slow elaboration. My ideas here are still premature. State or trait.
If this hypothesis is right, health care already have access to simple tools for early diagnosis and to find proper help for individuals. The brain is adaptable to changes, although it takes time (like dental brace) so it is possible to regain balance.
Maybe my intention is not fully explained. But balance between both eyes during development from newborn to grown up is what I am looking for. The developing brain.
3) Pharmacological treatment of post-traumatic stress syndrome, like soldiers who have experienced war (Vietnam war, Gulf war).
A. Is it possible to predict and monitor depression by measuring cortisol concentrations levels? Can β-blockers (not crossing the blood-brain barrier, ”heart-selective”, eg metoprolol) together with SSRI (sertralin) contribute to a rapid recovery and hampering of energy loss?
Depression (of course there are many subtypes of depression) is loss of energy.
However, the symptoms may vary a lot, also between man and woman. The cause of depression may depend on various external (eg stress) as well as innate factors. Your genes may carry a vulnerability, and therefore, you may be more sensitive/prone to develop depression. It should be noted that you can carry a genetic vulnerability during your lifetime, but depending on environmental factors you might develop or not develop a disease.
The reason why I believe heart selective β-blockers may be helpful is that it has been observed that patients might become more ”sensitive” after heart surgery. In particular men. A neural connection between the heart and the mesolimbic Dopamine-(acetylcholine?) system. There could be an adrenergic connection from the heart to mesolimbic area and/or vice versa.
This may be the connection between the heart and the soul. Interesting.
B. Sensitization and depression re-lapse.
Sensitization is eg, according to me, when the brain is more sensitive due to previous experiences/exposures. For example, this is very common in addiction. I believe that this also occurs in depression. This is closely connected to memory functions. Maybe that is why ECT sometimes is an alternative in treating depression. Here, studies are needed to define what sensitization is in depression. What external factors/environmental factors are involved?
C. Cytoprotection.
CNS Ca2+ sensitive channel blockers are useful in hampering symptoms at an early stage of depression.
Calcium is an ion that is extremely important for neural activity and communication in the brain. I believe that selective Ca-channel blockers can be useful in treatment of depression at an early stage. Depression should be divided into different types (like alcoholism is eg divided into problem drinkers, lonely drinkers, social drinkers etc). Different depressions need different treatments. Tailored treatment.
Ca channel blockers can be useful in regulating blood-pressure. However, I am not looking for these kind of blockers, rather selective Ca channel blockers for hampering action potentials in the central nervous system. The optimal pharmacological contribution would be to find out if the CNS has specific Ca channels which do not affect peripheral neuronal activity.