
 Svenska
Svenska
Category Archives: Uncategorized
Nu var det ett tag sedan jag skrev. Skriver på svenska ikväll. Statistiken visar att det är få besökare på min hemsida. Så det här blir ju en dagbok. En bok som jag delar mina tankar och funderingar med och som ingen läser, eller hur? 😉
Kvällens tema handlar om hur det är att leva som singel. Jag har varit singel i åtta år. Tiden flyger iväg. Visst har jag träffat män under den här tiden, men det är svårt att finna en soulmate på alla nivåer. Visst kan man tycka att jag har det bra, och det har jag. Men det finns dock känslor som inte kan ersättas med materiella ting eller pengar. En ledsamhet och tomhet. Jag är lycklig att jag har min utbildning som gör att jag kan hjälpa människor. Jag har räddat liv och minskat lidande för medmänniskor. Dessvärre har jag erfarenhet att människor kan vilja göra mig illa, väldigt illa. De vill önska mig allt ont som finns i hela världen. Varför förstår jag inte. Jag har oändligt många exempel.
De människorna har redan allt man kan önska sig; familj, hus, lyckliga liv etc. Så jag kan inte förstå varför de vill göra mig illa. Varför får jag inte leva mitt liv i fred?
Jag har en egenskap som jag är väl medveten om. Plikttrogenhet. Och den utnyttjas av andra. Jag tror inte att det är en förvärvad egenskap. Den är medfödd. Jag letar inte efter bekräftelse. Jag bekräftar mig själv genom att jag vet att jag har hjälpt medmänniskor. Det är en skyldighet.
Jag tänker ibland på hur det skulle vara att ha man och barn. Jag skulle vara som en lejon moder. Eftersom jag är människa så har jag fått möjligheten att intellektuellt styra mina handlingar. Det är dock svårt att inte låta sig påverkas av omgivningen. Subliminal perception är svår att undgå.
Det var söndagkvällens tankar.
Anna

I just wrote some on a research program. I like to have something to think about. To think about something else. Intellectual exercise. Theoretical science 🙂
Des bissous
Anna
——————————————-
“Je pense, donc je suis”
Descartes
——————————————–
If I would go back to research again, these would be the hypothesis’ I would work with. Research is not only to have a brilliant idea. It is also a huge work, at least in Sweden, to find founding for research. It costs a lot to run a lab etcetera. I was fortunate when I did my PhD. We had research grant from the NIH, and they carefully consider how to support research. If the reviewers find your research of interest and you get a research grant, you have to find evidence supporting your hypothesis. I must stress that it is not just to measure. You must have a reliable and stable method. And you also need ethical approval for your experiments. Very important. Yes, I have unfortunately experienced that data/ideas can be stolen and that is why I write this in public. These are, so far, only some ideas, so they are not true. Yet. They need to be tested before you can accept or reject.
1) Dopamine and -acetylcholine hypothesis
Dopamine is, according to me, the molecule of life. Giving life a meaning. A sense.
A value. It helps to send you signals if something is good or bad. Pleasure or punishment. Helps you to feel good. Helps you to survive.
But, after some life experience, I have noticed that balance is crucial. There should be something balancing dopamine, and here, acetylcholine can play an important role. This is very complicated since there are so many neurotransmitters and they are all important.
Smoking (and/or other forms of nicotine intake) is very common in several diseases. Professor Arvid Carlsson (Göteborgs Universitet, Sweden) hypothesised in the 1950’s that dopamine is involved in the pathophysiology of eg addiction (Engel and Söderpalm 1999; Yoshida et al 1980), schizophrenia and Parkinson’s disease (don´t know about Alzheimers disease). Smoking is highly observed among alcohol dependent individuals, depression and schizophrenia. These diseases are a huge burden for todays societies in terms of money, suffering, and not least, for families. During my years at the departement I always thought about why smoking is so common in several diseases.
Several experiments in vivo have demonstrated that dopamine plays a crucial role in these diseases. Professor Arvid Carlsson has further gained evidence for his hypothesis by introducing dopamine stabilisers. A pharmacological substance, with dual effects, acting as an agonist and antagonist depending on the state of the environment. (Since I write this from my memory, it may not be accurate). However, as seen in Parkinson´s disease, today´s available pharmacological treatment is not optimal. “On-off” symptoms may be observed. Dopamine neurons are widely distributed throughout the brain in rather distinct pathways. These neurons are closely located to eg cholinergic neurons. Cholinergic neurons have muscarinic (G-protein coupled) and nicotinic receptors (ion channels). To the best of my knowledge, dopamine neurons do not have ionic receptors. Maybe they are equipped with rapidly responding receptors, but they have not been found or simply: they do not exist. I don´t know the literature. A possible way to reduce side-effects may be to give more input to dopaminergic activity by cholinergic sparkling eg from the mesopontine area. These cholinergic neurons project to eg the ventral tegmental area and the substantia nigra. This is very difficult to study, that is why we don´t have the knowledge yet. Experiments will find out if dopamine and acetylcholine are like “Yin and Yang”. Opposites, stabilizing each other. Like an old fashion weight, and it is established that overweight is not good for health.
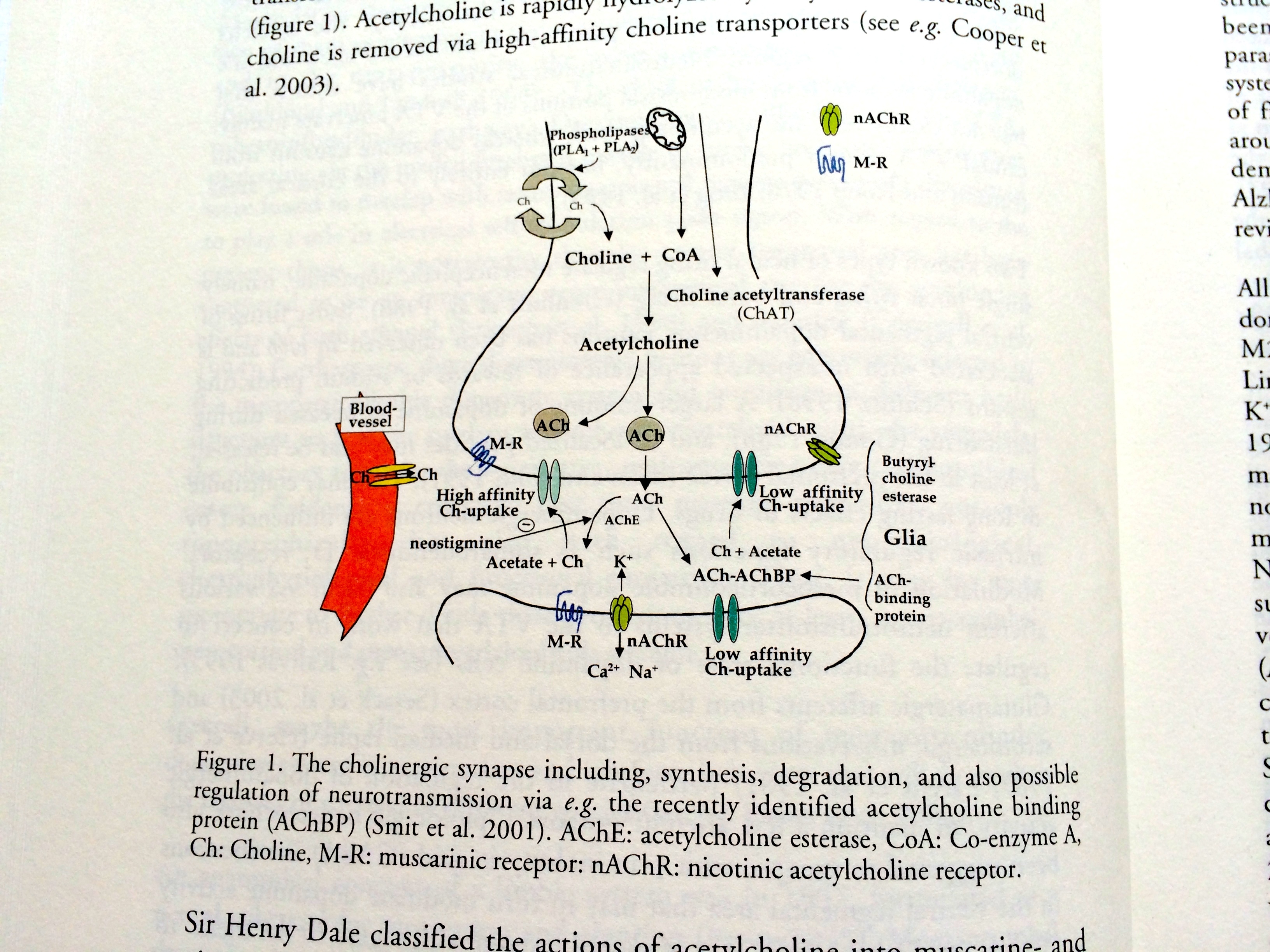
Above is an illustration of a cholinergic synapse. I have previously written about functional nicotinic acetylcholine auto receptors. These receptors should be introduced in this illustration pre-synaptically. To go further, I would suggest that these nicotinic receptors are composed by alpha-4 and beta-2 subunits.
It is interesting to note (now I write from my memory) that in Alzheimers disease, these subunits seem to be involved. Remember, this is theoretical pharmacology. A possible new pharmaceutical treatment could be to modulate this receptor. Acetylcholine esterase inhibitors are of clinically significantly importance so increasing acetylcholine activity could be of clinical significance.
B. Does dendritic dopamine overflow in eg substantia nigra interact with cholinergic neurons to give feed-back? A way to obtain balance between dopaminergic and cholinergic neurons.
2) Prevention of diseases in humans later in life is to monitor ophthalmological status in newborns – to obtain stability in our body.
Since I have read a lot about the brain in the literature a decade ago I have had time to reflect. I believe (a hypothesis that might be wrong) that the development of the ophthalmological nervous system is very important for the brain, our function (personality, decision making, motivation…) to be. Both “eyes” need to be in balance during development. If I remember correctly, the eye nerves cross in approximately in the middle of the brain and projects like a “spray” in the posterior. “Our function to be” is very difficult to define. Our personality, if it is allowed to have a personality.
This should be difficult to explain. Here, I feel, one should be very humble, and it needs careful and slow elaboration. My ideas here are still premature. State or trait. If this hypothesis is right, health care will get simple tools to diagnose early and find proper help for individuals. The brain is adaptable to changes, although it takes time (like dental brace) so it is possible to regain balance.
3) Pharmacological treatment of POST-TRAUMATIC STRESS SYNDROME, like in soldiers who have experienced war (Vietnam war, Gulf war).
A. Is it possible to predict depression by monitoring cortisol levels, and can beta-blockers (not crossing the blood-brain barrier, “heart-selective”, eg metoprolol) together with SSRI (sertralin) contribute to a rapid recovery and hampering of energy loss?
I have experienced depression and post traumatic stress syndrome and it is terrible. I still have flash backs of post traumatic experiences so I know exactly how veteran soldiers feel.
Depression (of course there are many subtypes of depression) is loss of energy. However, the symptoms may vary a lot. There are also differences between man and woman. The cause of depression may depend on various external (eg stress) as well as internal factors. Your genes may carry a vulnerability to be more sensitive/prone to develop depression. The reason why I believe beta-blockers may be helpful is that it has been observed that patients might become more “sensitive” after heart surgery (men become more sensitive?). A neural connection between the heart and the mesolimbic dopamine-(acetylcholine?) system. This is just some “brain-storming”. Not fully formulated hypothesis. There could be a adrenergic connection from the heart to mesolimbic area and vice versa of course.
To avoid side-effects, this is a working hypothesis, selective heart beta-blockers can be useful. This may be the connection between the heart and the soul.
B. Sensitization and depression re-lapse. Jag undrar om depression kan på något sätt försämra hjärnans funktion, alltså, utan depression är hjärnan ok, men en hjärna som varit med om en depression kan sensitiseras och därmed vara känsligare i framtiden. Det skulle eventuellt, den mycket välkända beta-blockeraren metoprolol hjälpa till att lindra. En låg dos kanske 25 mg dagligen. Om så är fallet, skulle det med en redan väl beprövad beta-blockerare kunna These questions need to be further explained.
C. CNS Ca2+ sensitive channel blockers are useful in hampering symptoms at an early stage of depression. Cytoprotection.
Calcium is an ion that is extremely important for neural activity in the brain. I believe that Ca-channel blockers can be useful in treatment of depression at an early stage. Depression should be divided into different types (like alcoholism is eg problem drinkers, lonely drinkers, social drinkers etc). Ca channel blockers can be useful in regulating blood-pressure. However, I am not looking for these kind of blockers, rather selective Ca channel blockers for hampering action potentials in the central nervous system. The optimal pharmacological contribution would be to find out if the CNS has specific Ca channels which do not affect peripheral neuronal activity.
I am soon turning 40 years. Yes, that is very true.
I previously wrote about my concerns about not having a family of my own. And I have to face the reality: that my life may turn out that way. Revealed that I have saved a few, very fragile, egg cells. However, it is extremely dangerous to believe that since I have saved some eggs that I will of course be able to have children later. This is definitely not a guarantee.
I feel very humble when it comes to biology. It is a fact that woman’s fertility dramatically decreases at the age of 35 and that age may contribute to health problems in children. I will not write more since this is not my field of knowledge.
This also generates a lot of thoughts. About life. But, I believe that as long as you don’t try to tell nature what to do, but rather find out and follow natures various “pathways”, you can live in harmony with nature. If you try to force nature, what will human life be in 10 generations?
Many sweet dreams,
Anna


Lång promenad
Eftertankens stund
Idag står tiden stilla.
Imorgon, en ny dag, men,
Same, same but…
/Allhelgonahelgen 2012